Social Worker First, Therapist Second
March is National Social Work Month, and every year I sit with this weird mix of pride and also the realization that some people don’t really believe social work is a real job. So let’s unpack (ha-ha therapisty term) what it means and how it shows up in my current work as a clinician.
A Little Background (Skip If You Already Know)
I didn't start out as a therapist. I started with a BSW, Bachelor of Social Work, doing child protection case management. Which means before I was ever sitting across from someone doing clinical work, I was helping people navigate systems and trying to help families find stability and safety. This would include things such as housing, benefits, food access, medical appointments, etc. It’s the unseen and unexciting stuff that doesn’t get recognized as “work” but is genuinely the difference between someone functioning day to day or not, or if they were stable enough to care for their child.
Then I went back, got my Addictions Counseling degree. Then I went back again, and got my Masters in Clinical Social Work. I got licensed and eventually moved into doing psychotherapy. I love this work but I didn’t just leave my case manager brain behind, and sometimes that part of me comes out (without me realizing it).
The Point of This
I was in supervision recently (yes, licensed clinicians still get supervision and consultation and they 100% should) and I was processing something that had been nagging at me afterwards.
I kept feeling this pull to fix things in a particular session. Therapists are basically taught specifically to not fix client problems, but help them solve it themselves. Internally I was having some psychoanalyzing of my own going on. Am I being too directive? Am I trying to fix the problem for them? Am I not holding the therapeutic frame? Am I doing therapy wrong?
My supervisor listened and then basically reflected back what I already knew but needed someone else to say out loud:
You're not trying to be a fixer.
You're recognizing what this person actually needs right now.
And she was right (she’s really good btw). Because this client at that particular moment in their life did not need to process their childhood wounds, they needed their basic needs met. Basic needs in the form of chronic stress, financial insecurity, disrupted sleep, and lack of support. I, in my very clinical therapist brain, was sitting there trying to do deep depth work with someone who was running on empty.
She brought up Maslow and I was like, “ahhhh yes,” Mr. Maslow.
Mr. Maslow. Stay With Me.
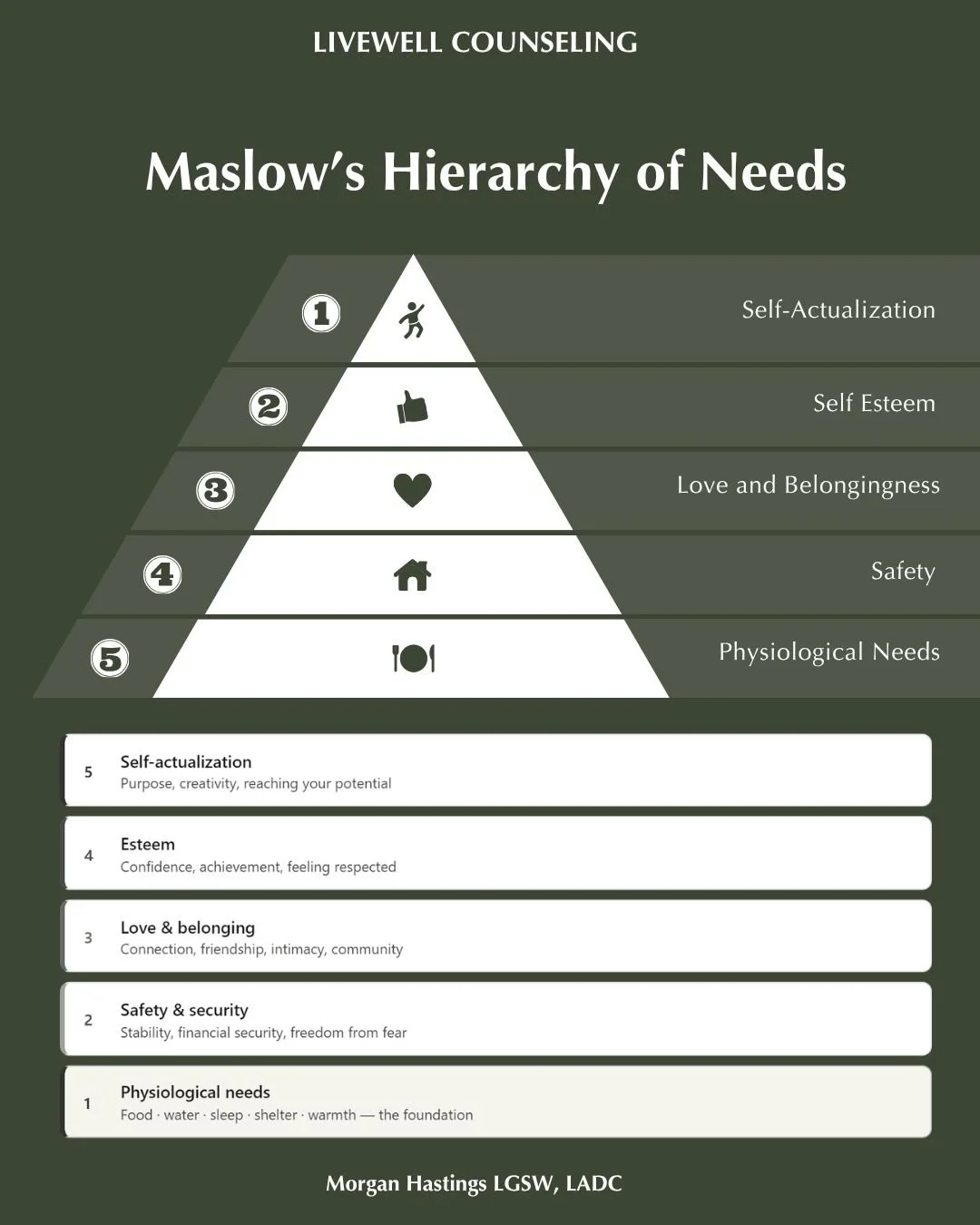
You've maybe seen the pyramid, and if not, Abraham Maslow proposed that human needs exist in a hierarchy. At the base: physiological needs which include food, water, shelter, sleep. Then safety. Then belonging. Then esteem. At the top: self-actualization.
Here's the part that gets lost when we apply this to therapy:
You cannot sustainably work on upper-level stuff when lower-level stuff is on fire.
This is just how humans work. I think it's one of the most important things to understand, not just in a therapy context, but about yourself if you've ever felt like you should be doing better and can't figure out why things aren't clicking. Or if you see people who don’t have their basic needs met and think, “why don’t they just get a job and work,” and it’s like brother, they don’t know where their next meal is coming from- let’s give them some grace. Side tangent, I digress.
The Foundation (kinda important)
Safe shelter, sleep, food, and financial stress don't exist in separate boxes. They compound each other, and the research is pretty hard to ignore.
Sleep is the one I see come up the most. When you're not sleeping (like really not sleeping, not just "I could use more" but running on fumes) your brain's ability to regulate emotion drops significantly. Increased anxiety, lower frustration tolerance, impaired decision making, and a nervous system stuck in a low-grade threat response. Some research even compares it to being in a "drunken" state. I personally experienced this myself during a period of serious burnout. I was slurring words, nodding off while driving. Scary stuff.
So the thing you came into therapy to work on? Your brain is too busy trying to keep you upright and functioning to process it.
Food is definitely underestimated, probably because we've been conditioned to treat eating as an afterthought rather than what actually runs the machine. Food is fuel, and our brain uses about 20% of your body's total energy. Skipping meals or surviving on whatever's fast and available hits your mood, concentration, and emotional regulation (sometimes before you even notice). Low blood sugar alone can look a lot like anxiety. Ever have too much caffeine on an empty stomach? Yeah, not a great feeling.
Financial stress gets the least clinical attention and deserves way more. In people that have financial stress or make high level decisions around money (like business owners, calling myself out), their money brain is always running in the background. It’s like working overtime on a problem that you can’t solve immediately, which leaves very little room for the reflection and processing that therapy asks of you. I would love to be able to provide financial counseling for this very reason- future thoughts.
It's the ultimate shit storm if I do say so myself. Poor sleep makes financial stress feel more catastrophic. Financial stress disrupts sleep. Sacrificing nutrition because money is tight or you are stressed out and overworked affects mood and cognition, which makes it harder to problem solve, which makes overall stress worse. They are one system, not three separate issues.
Why My Case Manager Brain is a Superpower
Social work has always been about the whole person in the context of their whole environment. “Person Centered Care” has been the backbone of this profession for over a century. It's why I will stop a session and ask about sleep, or ask about finances and budgeting. It might feel like I’m getting off track, but it’s so incredibly hard to get to the healing emotions part if those pieces aren’t addressed.
There's this unspoken hierarchy in mental health where clinical work gets treated as more sophisticated than case management or community-based work. I'd like to formally call that out as wrong. The skills I built before I had a clinical license such as systems navigation, understanding how poverty and instability actually affect mental health, and connecting people to what they actually need didn't become less relevant when I got my master's. They actually made me better at the clinical work (my supervisor pointed this out too, again she is great).
So Happy National Social Work Month
To every BSW doing case management wondering if what they're doing matters or counts, it counts way more than you know. You are often the reason someone's life doesn't completely fall apart and they’re able to keep going.
To every licensed clinician who sometimes feels the pull to problem solve and fix concrete things, trust it. Of course get consultation on it, but don't automatically pathologize it as a boundary issue.
To anyone in therapy who feels stuck or like they can't get to the “real stuff,” it might be worth asking what your foundation actually looks like right now. Things like sleep, food, safety, support, and stability are much more important. I make the occasional dark joke that if someone misses a session or feels like they didn’t get to the deep stuff with their time, that your childhood trauma isn’t going anywhere- so you can put it off for a little longer if you need to.
Don’t worry, we will get to self-actualization. Let's make sure you've eaten first.
your social work therapist,
Morgan